

What is IMO?
IMO is characterized by the presence of abnormal and excessive methanogenic archaea in the gastrointestinal (GI) tract, causing non-specific GI symptoms such as flatulence, abdominal discomfort, pain, and nausea. IMO is sometimes known as methane-dominant SIBO. Contrary to SIBO, which often has diarrhoeal presentations, IMO is associated with constipation (1, 2). It is estimated that at least 33% of patients with unexplained GI symptoms or those with irritable bowel syndrome (IBS) are affected by IMO (1).
Why does a high level of methane in the breath confirm IMO?
As hydrogen and methane gases are not endogenously produced by the human body but are the byproducts of microbial fermentation of undigested carbohydrates, they can serve as biomarkers for assessing methanogenic activity (3). Under normal physiological conditions, M. smithii, the most dominant methanogenic microbiome, plays a crucial role in the removal of hydrogen from fermented carbohydrates, which helps to enhance energy yield and ATP production of the host (4). With the hydrogen, M. smithii subsequently produces methane. When an overgrowth of M.smithii and other methanogens occurs, methane production increases, which correlates strongly with intestinal methanogen overgrowth (IMO) symptoms (5).
Receiving a diagnosis you’ve never heard of can be overwhelming. Intestinal Methanogen Overgrowth (IMO) is a condition that is often overlooked but can play a significant role in causing your gastrointestinal symptoms. In previous blogs, we provided an overview of IMO, covering its causes, diagnostics, and available treatments. In this one, we will guide you through the next steps after receiving a positive diagnosis.
What are my next steps?
As the pathophysiology and development of IMO can be multifaceted and complex, treatment involves targeting the underlying causes and addressing the symptoms. Here, we have largely broken down the next three steps.
Step 1: Identifying the underlying cause
Excess microbiome growth is usually limited by gastric acid, bile, peristalsis, and proteolytic digestive enzymes. However, there are conditions that impair these host defense mechanisms, fostering the overgrowth of microorganisms (6, 7):
| Anatomic abnormalities | Small intestinal diverticulosis, bowel structures, post-operative adhesions |
| Abnormal gastrointestinal motility | Irritable bowel syndrome (IBS), post-radiation enteropathy, hypothyroidism, diabetes mellitus |
| Compromised immunity defense | Immunodeficiency disorders, reduced IgA production |
| Reduced gastric acid production | Proton pump inhibitor use, autoimmune gastritis |
| Medications that slow transit | Opioids, anticholinergics, dopamine agonists, calcium channel blockers |
These conditions promote the overgrowth of archaea and slow gut transit, providing more opportunity for bacterial or archaeal action. Unfortunately, these conditions are chronic and challenging to cure, with many treatments offering only modest improvements in IMO symptoms. In addition, a clear indication is necessary to determine if the patient requires any operative or invasive intervention due to the risks involved.
Step 2a: Addressing the symptoms – antimicrobials and antibiotics
To address Intestinal Methanogen Overgrowth (IMO), your independent healthcare professional will design a targeted treatment protocol tailored to your specific breath data.
Many practitioners choose to begin with herbal antimicrobials to avoid the immediate use of pharmaceutical options and reduce the risk of antibiotic resistance. This can include specific botanical blends, prokinetics, and natural extracts like ginger and peppermint, which have been shown to be effective alternative options for managing overgrowths in some patients.
However, for stubborn or pronounced methane curves, pharmaceutical antibiotics are often required. Specifically, a combination of rifaximin and neomycin has been shown to be highly effective in alleviating GI symptoms and normalizing methane levels. In a clinical study evaluating this combination in patients with a positive methane breath test, 85% reported a strong clinical response. In comparison, only 63% and 56% of patients reported improvement when using neomycin or rifaximin as a standalone monotherapy (8).
Furthermore, in normalizing breath tests, 87% of subjects in the combination therapy group successfully eradicated methane, whereas only 28–33% of patients achieved methane elimination with single-antibiotic treatments (8).
The superior efficacy of rifaximin and neomycin is attributed to their unique behavior in the body—both are minimally absorbed by the systemic circulation, allowing their therapeutic actions to remain localized within the gut where the overgrowth resides (9). It is worth noting that because orally administered neomycin can carry systemic risks or face availability issues in certain regions, practitioners frequently pair rifaximin with alternative antibiotics like metronidazole depending on your location and clinical history (10, 11).
An Integrated Medical Safety Net
Because OMED Health operates on a strictly clinician-led model, your primary practitioner remains the architect of your recovery plan. However, if initial natural protocols fall short on a stubborn methane overgrowth, our platform features a built-in medical safety net. Your practitioner can seamlessly escalate your care, granting you direct access to an OMED Health medical doctor who can review your longitudinal breath curves and prescribe these targeted, localized antibiotic regimens—ensuring complete continuity of care.
Step 2b: Addressing the symptoms – the low FODMAP diet
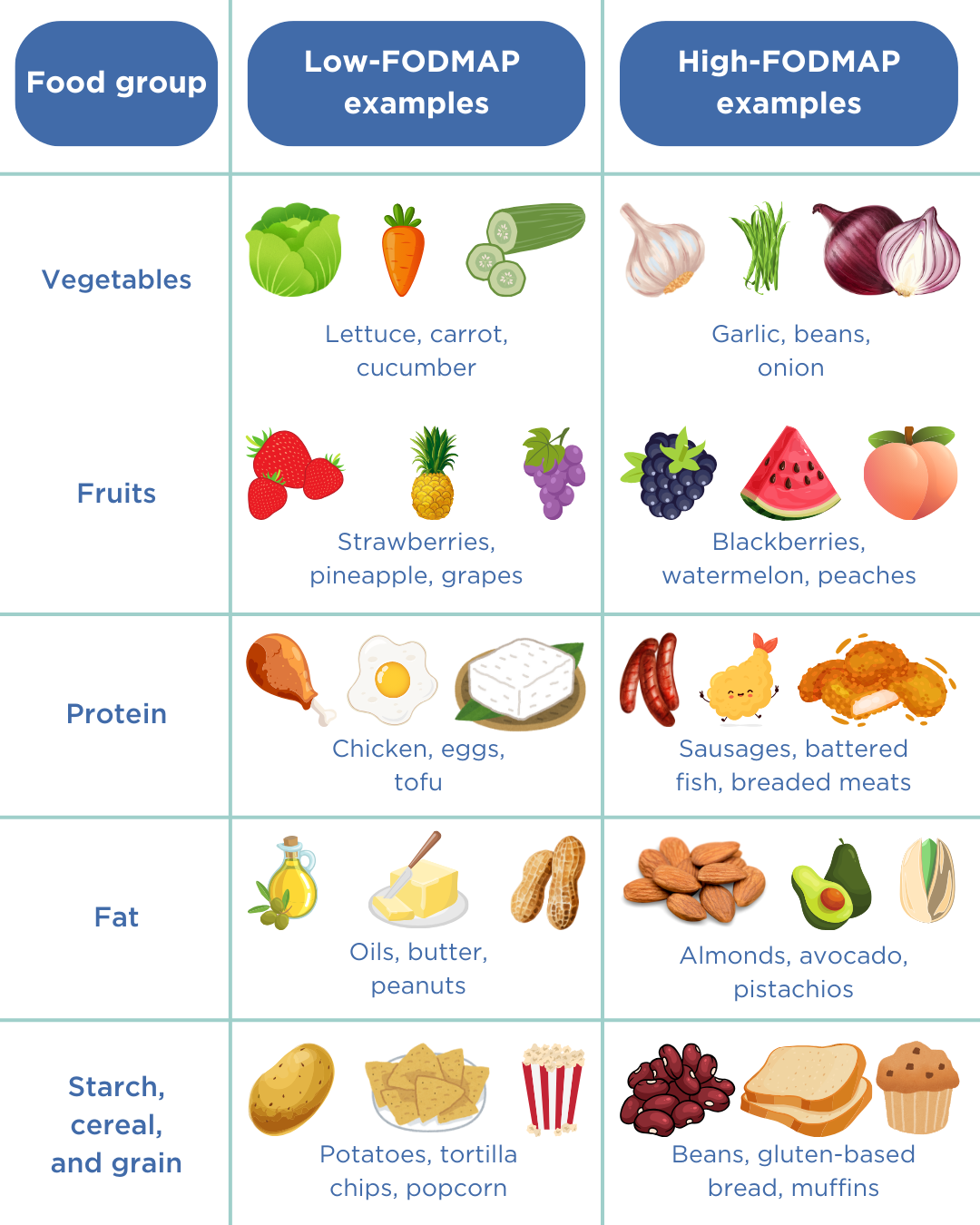
Another highly favourable and viable strategy for reducing symptoms during or after microbial treatment is the adoption of a low FODMAP (fermentable oligo-, di-, monosaccharides, and polyols) diet. FODMAPs are a group of short-chain carbohydrates that are poorly absorbed in the small intestine and are rapidly fermented by the gut microbiome, leading to gas production, water retention, and bloating. Limiting the intake of foods high in FODMAPs starves these microbes of their primary fuel source, limiting their growth and proliferation (16).
- High-FODMAP foods include: Certain dairy products (e.g., milk, yogurt, and ice cream), wheat-based products (cereal, bread, and crackers), and specific vegetables and aromatics (e.g., beans, lentils, onions, and garlic).
- Low-FODMAP foods include: Eggs, meat, specific grains (e.g., rice, quinoa, and oats), and select vegetables (e.g., aubergine, potatoes, and tomatoes) (17).
The effects of a low-FODMAP diet exhibit considerable inter-patient variability, meaning that different individuals experience vastly different responses to the same foods. Because completely eliminating these foods long-term can lead to nutrient deficiencies and negatively impact your beneficial microbiome, the low FODMAP approach should be used as a temporary diagnostic tool under your practitioner’s guidance. The standard structured approach involves:
- Elimination: Adhering strictly to the low FODMAP diet for 4–6 weeks to determine if symptoms improve.
- Reintroduction: Systematically reintroducing one high-FODMAP food group at a time while observing symptoms over a three-day window.
- Personalization: Establishing a long-term, balanced diet that incorporates your specific tolerated threshold of high-FODMAP foods (18).
Step 2c: Addressing the symptoms – the elemental diet
In exceptionally severe or treatment-resistant cases, your practitioner may discuss an alternative approach known as the elemental diet. This involves a medical meal-replacement formula containing completely pre-digested nutrients, vitamins, and minerals. Because the components are so simple they can be absorbed almost immediately in the very upper parts of the digestive tract, the elemental diet meets all of the host’s nutritional requirements while simultaneously starving the microorganisms residing further down the small intestine (12).
Studies by Pimentel et al. (2004) and Rezaie et al. (2024) found that a 2-week elemental therapy window was effective in normalizing lactulose breath tests in 58–100% of IMO patients. Even in cases where methane was not entirely eliminated, many individuals still showed a significant reduction in maximum exhaled methane levels and peak hydrogen rise (13, 14).
However, because elemental diets are highly restrictive and are often associated with poor palatability, compliance can be challenging, and long-term data remains limited (15). This intervention requires close clinical supervision, so it is essential to discuss it thoroughly with your healthcare provider.
Step 3: Preventing Remission and Long-Term Surveillance
Because initial treatments focus primarily on reducing the immediate microbial overgrowth, IMO has a high rate of recurrence, particularly in individuals with underlying motility issues or chronic conditions that predispose them to excessive microorganism growth.
Successfully managing IMO over the long term requires precision and timely intervention before a full relapse occurs. This is where continuous tracking becomes invaluable.
The medical-grade OMED Health Breath Analyzer, which patients use during their 12 week clinician-guided testing window, serves as a powerful surveillance tool. By using the device in conjunction with the OMED Health App to log daily food intake and symptoms, you and your practitioner can systematically monitor exactly how your gut microbiome is reacting post-treatment. If your IMO has been resolved, your practitioner can utilize routine, targeted testing loops to catch early gas spikes and adjust your maintenance protocol before symptoms take over.
Conclusion
While the treatment of IMO largely involves balancing these three steps, considerable inter-patient variability exists. There is no one-size-fits-all cure. Tailoring a treatment regimen to align with your unique data, lifestyle, and clinical history is essential for achieving the most effective and sustainable outcomes.
By working directly with an approved healthcare professional utilizing the OMED Health platform, you secure a data-driven path to recovery, backed by a medical safety net every step of the way.
References
- Rezaie A, Rao SSC. Chapter 15 – Intestinal bacterial, fungal, and methanogen overgrowth. In: Rao SSC, Parkman HP, McCallum RW, editors. Handbook of Gastrointestinal Motility and Disorders of Gut-Brain Interactions (Second Edition) [Internet]. Academic Press; 2023 [cited 2024 Sep 5]. p. 205–21. doi: 10.1016/B978-0-443-13911-6.00015-3
- Mehravar S, Takakura W, Wang J, Pimentel M, Nasser J, Rezaie A. Symptom profile of patients with intestinal methanogen overgrowth: A systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2024 Aug 10;S1542-3565(24)00716-X. doi: 10.1016/j.cgh.2024.07.020
- https://www.bsg.org.uk/clinical-resource/agip-protocol-for-hydrogen-methane-breath-testing
- Mohammadzadeh R, Mahnert A, Duller S, Moissl-Eichinger C. Archaeal key-residents within the human microbiome: characteristics, interactions and involvement in health and disease. Current Opinion in Microbiology. 2022 Jun 1;67:102146. doi: 10.1016/j.mib.2022.102146
- Yao CK, Tuck CJ. The clinical value of breath hydrogen testing. Journal of Gastroenterology and Hepatology. 2017;32(S1):20–2. doi: 10.1111/jgh.13689
- Sorathia SJ, Chippa V, Rivas JM. Small Intestinal Bacterial Overgrowth. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Feb 28]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK546634/
- Tansel A, Levinthal DJ. Understanding Our Tests: Hydrogen-Methane Breath Testing to Diagnose Small Intestinal Bacterial Overgrowth. Clin Transl Gastroenterol. 2023 Feb 3;14(4):e00567. doi: 10.14309/ctg.0000000000000567
- Low K, Hwang L, Hua J, Zhu A, Morales W, Pimentel M. A combination of rifaximin and neomycin is most effective in treating irritable bowel syndrome patients with methane on lactulose breath test. J Clin Gastroenterol. 2010 Sep;44(8):547–50. doi: 10.1097/MCG.0b013e3181c64c90
- Algera JP, Törnblom H, Simrén M. Treatments targeting the luminal gut microbiota in patients with irritable bowel syndrome. Current Opinion in Pharmacology. 2022 Oct 1;66:102284. doi: 10.1016/j.coph.2022.102284
- Veirup N, Kyriakopoulos C. Neomycin. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Sep 5]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK560603/
- Neomycin sulfate | Drugs | BNF content published by NICE [Internet]. [cited 2024 Sep 5]. Available from: https://bnf.nice.org.uk/drugs/neomycin-sulfate/
- Nasser J, Mehravar S, Pimentel M, Lim J, Mathur R, Boustany A, et al. Elemental Diet as a Therapeutic Modality: A Comprehensive Review. Dig Dis Sci. 2024 Jul 13; doi: 10.1007/s10620-024-08543-1
- Pimentel M, Constantino T, Kong Y, Bajwa M, Rezaei A, Park S. A 14-Day Elemental Diet Is Highly Effective in Normalizing the Lactulose Breath Test. Dig Dis Sci. 2004 Jan 1;49(1):73–7. doi: 10.1023/B:DDAS.0000011605.43979.e1
- Rezaie A, Chang BW, Houser K, Mathur R, Brimberry D, Rashid M, et al. Mo1359 COMPLIANCE, SAFETY, AND EFFECT OF EXCLUSIVE PALATABLE ELEMENTAL DIET IN MICROBIAL OVERGROWTH: A PROSPECTIVE CLINICAL TRIAL. Gastroenterology. 2024 May 18;166(5, Supplement):S-1039. doi: 10.1016/S0016-5085(24)02863-4
- Achufusi TGO, Sharma A, Zamora EA, Manocha D. Small Intestinal Bacterial Overgrowth: Comprehensive Review of Diagnosis, Prevention, and Treatment Methods. Cureus. 12(6):e8860. doi: 10.7759/cureus.8860
- FODMAP Diet: What You Need to Know [Internet]. 2021 [cited 2024 Sep 5]. Available from: https://www.hopkinsmedicine.org/health/wellness-and-prevention/fodmap-diet-what-you-need-to-know
- nhs.uk [Internet]. 2018 [cited 2024 Sep 5]. Irritable bowel syndrome (IBS) – Further help and support. Available from: https://www.nhs.uk/conditions/irritable-bowel-syndrome-ibs/further-help-and-support/
- Starting the Low FODMAP Diet – Monash Fodmap [Internet]. [cited 2024 Sep 5]. Available from: https://www.monashfodmap.com/ibs-central/i-have-ibs/starting-the-low-fodmap-diet/

